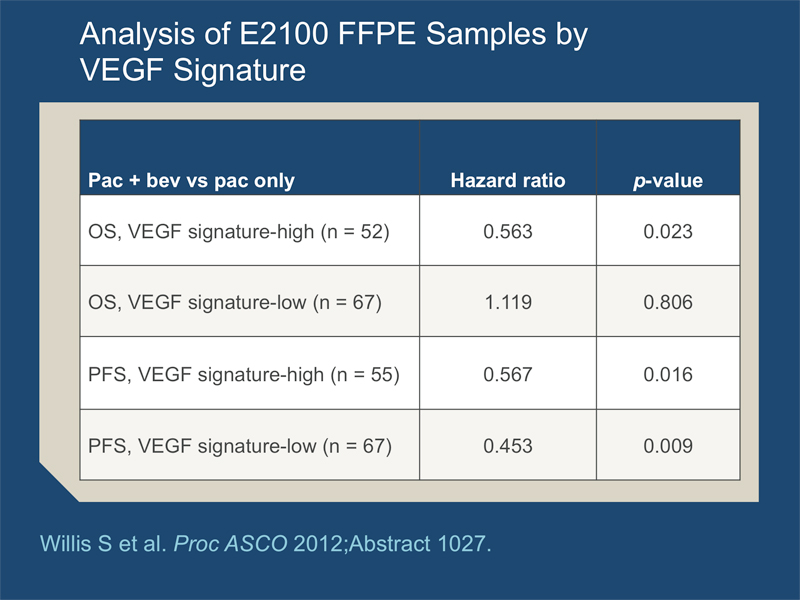
- This tumor assay on 122 patients in E2100 predicted OS benefit from Bev. However, this work is exploratory and underpowered.
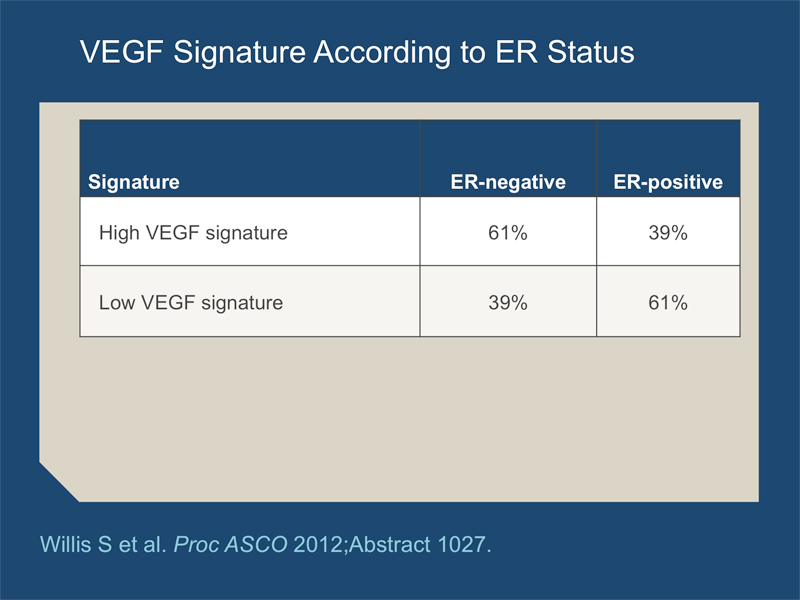
- VEGF signature level is inversely correlated with ER. Further investigation continues.
As part of a recent case-based CME initiative developed by our group, oncologist Dr Alan Astrow of Brooklyn, New York presented a 56-year-old woman from his practice with a triple-negative tumor and disease recurrence in the sternum and regional nodes. Because no other disease was present she received treatment with the slim objective of “cure,” and since this was in 2008 Dr Astrow used bevacizumab and nab paclitaxel followed by regional radiation therapy. Improbably, the patient currently remains off treatment, disease free and feeling very well. Dr Astrow fully understands that the same extraordinary outcome might have resulted from weekly paclitaxel followed by radiation therapy or radiation therapy alone, but he presented this case to gain greater understanding of whether select patients derive particular benefit from specific treatments — for example, bevacizumab in triple-negative disease. This poster presented at ASCO addressed this question by reporting on a 13-gene VEGF signature associated with cellular response to hypoxia in tumor samples obtained from patients in the classic ECOG-E2100 trial of bevacizumab/paclitaxel in metastatic disease. Interestingly, based on this retrospective evaluation a survival benefit is observed only in patients in the “high” signature group. Unfortunately, this assay and others evaluating a variety of potential predictors of response to bevacizumab seem pretty far from “prime time,” and this anti-VEGF agent remains off the shelf even with the knowledge that individual patients who might experience profound treatment benefit are not now able to receive it.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}